

The Next Latex: The Allergy Hiding in Plain Sight
Chlorhexidine is the antiseptic almost everyone in American medicine meets and almost no one tracks — and that gap, not its rarity, is the danger.
By Kenneth Hoffmann and Katherine Hoffmann Goldsword, Founders, Hoffmann Goldsword Foundation
If you have surgery in the United States, there’s a good chance the last thing to touch your skin before the first cut will be chlorhexidine — the antiseptic scrubbed over the surgical site, soaked into the wipes sent home the night before, swabbed into mouths, coated onto catheters and dressings. It’s used on tens of millions of patients a year, and for almost all of them it does exactly its job: it lowers the risk of infection.¹
For a smaller and growing number, the immune system quietly turns on it. The sensitivity is usually acquired — built through repeated, ordinary exposure — and it tends to give no warning until the encounter that sets it off. That is what happened to Katherine. During a routine spinal fusion in October 2024, her blood pressure crashed and her heart stopped. It wasn’t the surgery, and it wasn’t the anesthesia. It was the antiseptic. She had no recorded allergy to it; the cause was confirmed only afterward, through allergy testing.²
Her case is documented in detail — and what’s striking isn’t that it happened to her. It’s how easily a reaction like it goes unrecognized, uncounted, and unprevented. We went looking for how often chlorhexidine does this, how the system tracks it, and what stops the next one, and we kept arriving at the answer that should unsettle you most: mostly, it doesn’t. The system was never built to see it.
This is not a story about a rare allergy. It’s about a danger that is real, growing, and effectively universal — one hiding inside a number that looks reassuringly small only because almost no one is counting. Here is what we found.
A danger you acquire, not one you’re born with
Most people picture an allergy as something fixed — a trait you’re born with, a line drawn at birth between the few who have it and the many who don’t. That picture is exactly what makes chlorhexidine easy to underestimate, because the reaction it can provoke doesn’t work that way.
Chlorhexidine hypersensitivity is, in most cases, acquired. The immune system isn’t born primed against it; it learns. With repeated exposure, some people begin building a response to a molecule they once tolerated, and that process can run silently for a long time — no rash, no warning, no hint that a threshold is being approached.³ The sensitivity that results can stay invisible until a single later encounter sets off a reaction out of all proportion to anything before it. By the time there is a “first symptom,” it can be anaphylaxis.⁴
For the person it’s happening to, none of this registers. Each exposure feels like nothing — a swab before an IV, a rinse at the dentist, a wash before a procedure — routine events done without incident and forgotten. There’s no escalating signal, no tally being kept. Sensitization, as it develops, leaves nothing the patient can feel, which is why the eventual reaction so often arrives as a complete surprise.
That changes who is at risk. If the danger were inborn, it would belong to a small, identifiable group who could, in principle, be warned. Because it’s acquired through exposure, the at-risk group is defined by exposure instead — and exposure to chlorhexidine is nearly universal in modern care. It’s the standard surgical skin prep, the pre-operative wipe patients are sent home with, the mouthwash and dental rinse, the coating on catheters and central lines, the antiseptic in wound dressings.² Most people meet it many times over a lifetime of ordinary medical encounters, almost always without learning its name. The population quietly accumulating exposure isn’t a niche; it’s functionally everyone who passes through a hospital. And the case literature suggests this is happening more, not less, often.²
There’s also a way ordinary people, doing an ordinary thing, increase how much of it their bodies take in.
Chlorhexidine is absorbed through the skin, and intact skin is a fairly good barrier. Disrupted skin is not. Freshly shaved or waxed skin — nicked, abraded, its surface stripped — absorbs more of whatever is applied to it. This isn’t a contested point; it’s one of the explicit takeaways of the peer-presented case at the center of this piece, whose authors note that applying chlorhexidine to shaved or injured skin risks increasing absorption.²
The trouble is that shaving or waxing before a procedure isn’t discouraged — it’s common, sometimes expected, and the standard instructions that come with a pre-operative chlorhexidine wash say nothing about it. A patient told to wipe down with the antiseptic the night before and the morning of surgery may reasonably shave first, the way people do before any occasion, and in doing so hand the chlorhexidine an open door — without ever being told the two don’t mix. That is what Katherine did. Following the standard preparation, she shaved, then used the chlorhexidine wipes she’d been given; the wipes burned, and a hive-like rash rose where she’d applied them.²
None of this means a shave is what makes someone allergic, or that intact skin is safe — chlorhexidine reaches the body through many routes, and a person already sensitized can react to a mouth swab or a coated catheter with no skin involved at all. The point is narrower and sturdier: a disrupted barrier increases the dose, the dose is one of the few variables a patient actually controls, and nothing in the system currently tells them so. A small, free, avoidable amplifier, sitting in plain sight — which is the first glimpse of the pattern that runs through everything ahead. The danger is ordinary, it’s widespread, and the system around it isn’t paying attention.
Recognition without protection
The danger is not unknown. Chlorhexidine allergy has its own literature — narrative reviews, case series, specialist guidance — and the substance carries warnings in more than one country. If the problem were simply that medicine had never noticed, it would be smaller, and far more solvable. Recognition, in the sense of documented somewhere by someone, already exists. It has not been enough.
The reason is that recognition and protection are not the same thing, and the distance between them is where patients get hurt. Knowledge of chlorhexidine’s risk lives where knowledge accumulates — journals, reviews, the experience of allergists who have seen a case. It does not reliably reach the place and the moment exposure happens: the prep tray, the wipe handed to a patient the night before surgery, the opening minutes of an operation. A risk can be well established in the literature and operationally invisible at the bedside at the same time. That coexistence is the whole problem.
It begins at the moment of the reaction itself, which the system frequently fails to recognize for what it is. When the United Kingdom’s Royal College of Anaesthetists ran its large national audit of life-threatening allergic reactions during surgery, chlorhexidine emerged as one of the leading culprits — and yet it was suspected in only about a quarter of the cases later confirmed to be caused by it.⁵ In three of every four confirmed cases, the clinicians watching the reaction unfold did not initially think of the antiseptic. When the cause isn’t recognized as it happens, it isn’t recorded as chlorhexidine, isn’t learned from, and may never be communicated to the patient who just survived it. The failure to see starts at the bedside and propagates outward.
And it keeps failing at every step after the bedside. Suspecting chlorhexidine is not the same as confirming it: confirmation takes a specialist skin-prick and intradermal workup that isn’t available everywhere, isn’t uniformly done, and that most patients never get. A reaction that is finally proven then meets the next gap: it still can’t be counted. Chlorhexidine allergy has no diagnostic code of its own; it disappears into generic headings like “allergy to other drugs,” where it can’t be tallied or pulled back out. And nothing sits above any of this, actively watching. The United States learns of these reactions through voluntary, after-the-fact reports — a system that catalogs what happens to be sent in, not one that goes looking — and it has never run the kind of active national surveillance that, in other countries, is exactly what made the true scale visible. Each empty layer guarantees the next stays empty: unrecognized reactions are never confirmed, unconfirmed ones are never counted, and what is never counted never prompts anyone to look. The blindness here isn’t one gap. It is a stack of them — and in the United States it runs especially deep.
That last point is not a guess; it is visible in how differently the rest of the world has treated this. Regulators abroad have been warning about chlorhexidine for four decades. Japan’s health ministry advised against putting it on mucous membranes as early as 1984, and in the years that followed, drug-safety agencies in Norway, France, the United Kingdom, and Australia issued their own alerts about severe reactions to the antiseptic and to the devices that contain it.³ Britain went furthest, funding the active national audit that identified chlorhexidine as a leading surgical allergen in the first place — the kind of deliberate, go-looking surveillance no American agency has ever mounted for this.⁵ The United States, by contrast, issued a narrow device notice in 1998 and a consumer-label change in 2017, and otherwise left the counting to whatever happened to be reported.³,⁸ The danger is the same on every side of every border. What differs is whether anyone decided to look.
Suppose it is recognized and written down. Even then, documentation is a record, not a control. An allergy noted in a chart is information; it is not a brake on the machinery. The decisions that determine which antiseptic actually touches a patient — which prep is on the tray, which wipe protocol the floor uses, which catheter is stocked — run on defaults and routines, not on someone pausing to read the allergy list at the instant of exposure. An alert can sit in the record while the standard prep proceeds, because the standard prep is what happens by default, and the exposure comes first. The note and the action live in different worlds.
That gap is widest precisely where exposure is most likely: the start of care. Skin antisepsis, line placement, oral swabs, dressings — front-loaded into the opening minutes, performed before a full history is reviewed and sometimes before the patient can speak. In an emergency, the window to check anything collapses to nothing. So a patient whose chlorhexidine allergy is fully documented can still be exposed again — not through carelessness, but because exposure is built into the beginning of the process, ahead of the point where the documented knowledge could act.
And the risk travels badly. Sensitization is permanent: once a person reacts, they are at risk for life, in every setting that uses the substance. But the systems meant to carry that fact forward aren’t built to hold it as a durable, high-priority constraint. A flag visible in one clinic’s record may not survive a transfer to another hospital, a new electronic system, a different specialty, a span of years. What is actionable in one place quietly goes invisible in the next. A lifelong hazard is being tracked by infrastructure designed for episodes.
It would be easier, in a way, if this all came down to a careless person or a negligent institution — someone to name, correct, replace. It doesn’t. These are the ordinary failure modes of complex systems, documented across safety-critical fields for decades: harm emerges not from one bad decision but from many locally reasonable ones that fail to line up, in environments where no single participant sees the whole chain.⁶ Each clinician follows the protocol in front of them; each protocol is defensible alone; the patient is harmed in the seams between them. This isn’t an excuse for the system — it’s the diagnosis of it. And it carries a hard implication: a problem produced by structure is not solved by individuals trying harder. It is solved only by changing the structure — the defaults, the records, the way risk is carried from one moment of care to the next.
That is the shape of the blindness in the abstract: recognized in principle, unseen in practice, un-acted-upon where it counts, unable to follow the patient through time. Stated that way it can sound almost bloodless. It is not. To see what it costs, it helps to watch it operate once, in full, on a single documented case — one severe enough to leave no doubt that something nearly killed her, where naming what did took a workup most patients never get.
“The note and the action live in different worlds.”
One case, in full

We’ve described the danger and the blindness in general terms. Here is what they looked like in one body, on one morning — the case at the center of this piece, and the reason we know it from the inside. Katherine is one of the two of us writing this. What follows is drawn from her medical record and from the case the physicians who evaluated her presented, in anonymized form, at a national allergy and immunology meeting — not from memory.
In October 2024, Katherine went in for a cervical spinal fusion, a planned operation to relieve pressure on her spinal cord. She had no recorded allergy to chlorhexidine. Like patients everywhere, she’d been given antiseptic wipes to clean her whole body the night before and the morning of surgery, and — as people do — she had shaved beforehand. The wipes burned where she applied them, and a hive-like rash came up on her skin.²
That was the opening of a cascade, not the whole of it. In the pre-operative area she used the wipes again. Then, as the operation began, the chlorhexidine kept arriving — in the antiseptic prep for an arterial line, in the dressing taped over it, in a throat spray once she was intubated, and, in the intensive care that followed, through a central line, a urinary catheter, and mouth swabs.²,⁷ None of it registered as one large dose, because it wasn’t; it was many exposures, through skin, mucous membrane, and the bloodstream’s access points, layered over a barrier already stripped by shaving. Shortly after the drugs that begin anesthesia were given, her heart went into pulseless electrical activity — a form of cardiac arrest. It took about ten minutes of resuscitation to bring her back.²
The cause was not obvious, and that is the part that matters. The arrest had followed a muscle relaxant given moments earlier — the usual first suspect in an operating-room collapse — and no antibiotics, the other usual suspect, had been given at all.² A case like this could easily be recorded as an anesthetic reaction of unknown cause; many are. What pinned it instead was a workup most patients never receive. An allergy and immunology clinic tested her systematically: skin-prick testing for both the muscle relaxant and chlorhexidine came back negative, and the muscle relaxant was cleared on deeper intradermal testing too — but intradermal testing for chlorhexidine turned strongly positive.²,⁷ The confounder was excluded and the culprit named. The diagnosis didn’t coast through on a guess; it survived the obvious alternative.
The record holds one more truth we won’t smooth over. The assessment was chlorhexidine allergy together with a likely underlying mast-cell component, her tryptase running persistently at the upper edge of normal in the months afterward — while a genetic test for the inherited form of that trait came back normal.²,⁷ We state both halves plainly, because a careful reader deserves them: she was not a person with no risk factors, and she was also not someone carrying an inborn condition that made her a special case. What nearly killed her is the danger available to almost anyone — an acquired sensitivity, surfacing through ordinary, compounding exposure.
She survived, and now lives inside a permanent constraint. Her physicians have judged the allergy severe and life-threatening and advised her to avoid chlorhexidine in every form — not only in surgery but in dental care and routine medicine — because any future exposure carries the risk of another severe reaction.⁷ One of the most common antiseptics in American medicine is now, for her, something that must be kept out of every room she is ever treated in, for the rest of her life.
That is easier to write than to live. The substance she has to avoid is nearly everywhere care happens — the scrub before surgery, the wipe before a blood draw, the rinse at the dentist, the coating on a catheter, the gel on an instrument. Avoiding it is not one decision made once; it is a small, constant act of vigilance attached to every appointment, every procedure, every unfamiliar room, indefinitely — the work of staying ahead of a hazard that the system around her does not reliably track on her behalf. She is, in effect, holding the line the system doesn’t. That is part of why her name is on this piece. The point of telling her story is not that it happened to her; it is that the gap that nearly killed her is still open for the next person, who will not know to watch.
Hold the whole sequence in mind. A documented, near-fatal reaction during surgery. A confounder actively excluded and a culprit confirmed by testing. A patient with a named diagnosis and a written instruction that the substance is life-threatening to her. If the system is going to recognize chlorhexidine anywhere, it should recognize it here — in the most thoroughly worked-up case it is ever likely to see. And even here, naming the cause took months of deliberate specialist effort, after the arrest rather than before it.
Which leaves the question this case forces — the one the next section answers. If a reaction this severe, this documented, this carefully diagnosed was still this hard to see for what it was, how many are never seen at all?
“She is, in effect, holding the line the system doesn’t.”
The gap in the numbers
So how often does this actually happen? The official answer is the reason chlorhexidine reactions are called rare — and it deserves a close look, because it’s the number that has done the most to keep the danger invisible.
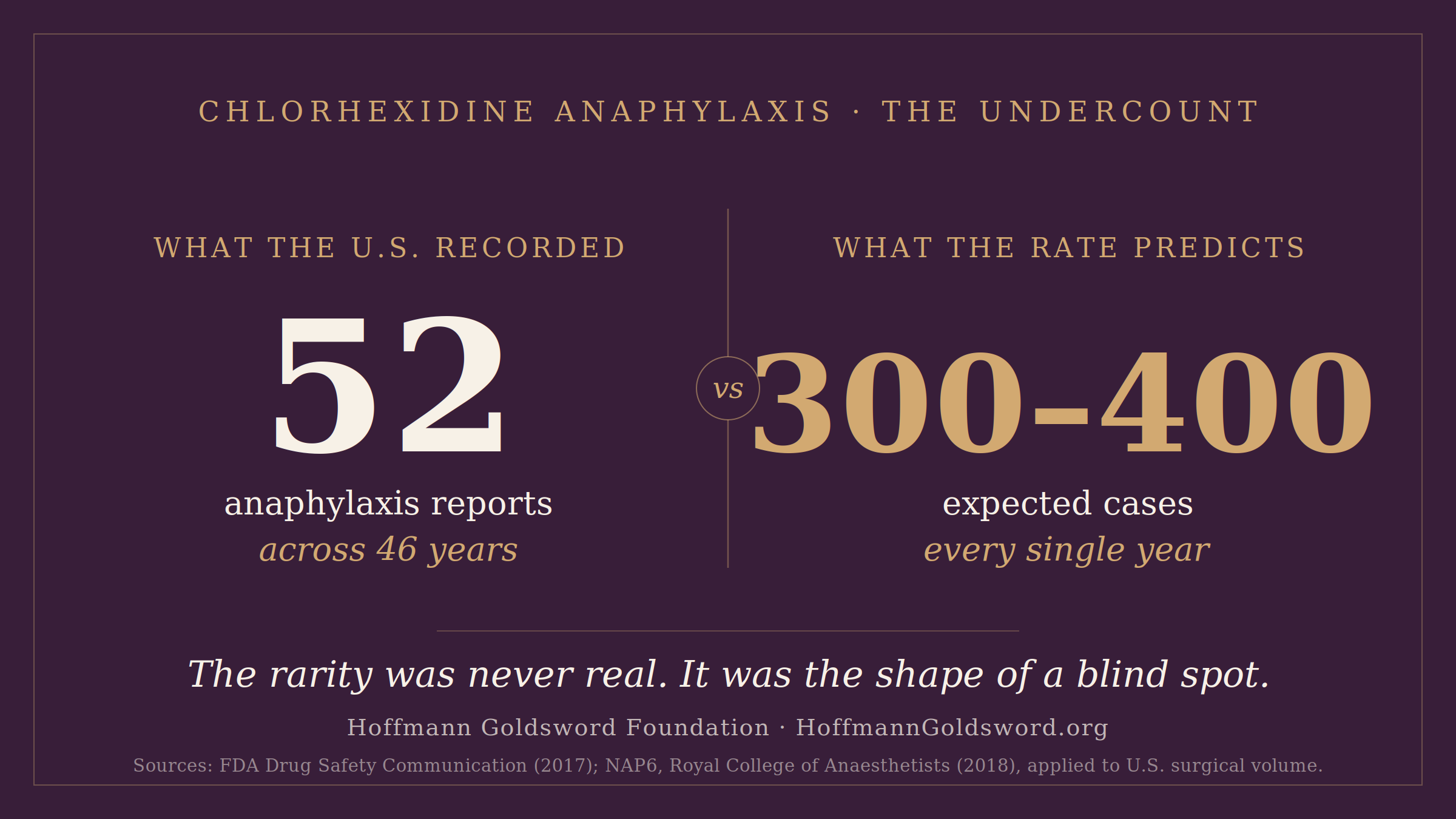
In 2017, after reviewing decades of data, the U.S. Food and Drug Administration warned about serious allergic reactions to skin-applied chlorhexidine. The basis was a tally: 52 reports of anaphylaxis to topical chlorhexidine between 1969 and 2015 — 43 of them drawn from the agency’s adverse-event reporting system — two of them fatal.⁸ Fifty-two cases in forty-six years. Set against the tens of millions exposed annually, a number that small reads as reassurance. It is the statistical bedrock of “rare.” And even inside it, the trend points one way: more than half of those cases were reported after 2010, the curve bending upward even as the system barely registered it.⁸
Now hold it against what the rate predicts. When the United Kingdom’s Royal College of Anaesthetists went actively looking — auditing serious surgical anaphylaxis nationwide rather than waiting for reports — chlorhexidine caused about 9% of cases, the third most common trigger of life-threatening allergic reactions during surgery.⁵ From that audit one can derive an approximate per-exposure incidence, on the order of 0.78 cases per 100,000 exposures. Apply it to the 40 to 50 million surgical procedures performed in the United States each year,¹ and the expected number lands in the range of 300 to 400 cases annually.
Not over forty-six years. Every year.
That projection is a model, and it deserves its caveats. The underlying rate may run high; the FDA’s count was limited to skin-applied chlorhexidine and to what got voluntarily reported; perioperative anaphylaxis and topical-product reports do not measure exactly the same thing. Grant all of it. Be as conservative as the evidence allows, cut the estimate by more than half, and the two numbers still don’t live in the same world. Dozens of cases across five decades cannot be reconciled with hundreds expected in a single year by definitions and caveats alone. The gap is too many orders of magnitude wide. Something other than the true frequency is being measured.
What’s being measured is detection. A recorded case requires a chain to succeed at every link: the reaction recognized as anaphylaxis, the anaphylaxis attributed to chlorhexidine, the attribution written down as chlorhexidine, and a report actually filed. We’ve already seen where that chain breaks — in the same audit, chlorhexidine was suspected in only about a quarter of the cases it caused.⁵ The other three-quarters were something else in the record: an anesthetic reaction, an unspecified anaphylaxis, a cardiac event. Most hospitals have no standard way to code a chlorhexidine allergy at all. A reaction never attributed is never reported, and a case never reported never happened, as far as the data is concerned. The 52 isn’t a measure of how often chlorhexidine nearly kills someone. It’s a measure of how often the system manages to notice.
Set the two numbers side by side one more time. Modeling from how often this happens during surgery places the real figure in the hundreds of cases a year. The official record holds a few dozen across half a century. The rarity is not a property of the danger; it’s a property of the measurement — an artifact of a system that cannot see what it does not code, count what it does not attribute, or report what it never recognized. The silence in the data has never meant the danger is small. It has only ever meant we weren’t looking.
And there is one more reason that silence should alarm rather than comfort. We’ve watched a ubiquitous medical material sensitize a mass population in plain sight before — and we know how that story ends.
“Not over forty-six years. Every year.”
The next latex
We keep saying this is not the first time, so let us be plain about what we mean. A generation ago, another material almost everyone in a hospital touched turned, on a mass scale, into something that could harm the people it was meant to protect.
As universal precautions against bloodborne infection took hold after 1987 — medicine’s response to HIV and hepatitis — the use of latex gloves and other devices climbed steeply, and exposure to natural rubber latex became, in effect, universal across medical care. What followed wasn’t a handful of unlucky reactions; it was an epidemic of acquired sensitivity. And it was driven by a detail almost no one was watching: most gloves were dusted with cornstarch to make them easier to pull on, the powder picked up latex proteins, and every time a pair was snapped on or stripped off, those proteins went into the air. Operating rooms turned out to hold the highest airborne latex concentrations anywhere in the hospital — people were being sensitized not only through their hands but through the air they breathed at work. At the peak, by some estimates, up to 17% of health care workers had become allergic, and among the patients with the heaviest lifetime exposure — children with spina bifida, who face repeated surgery from birth — the rate ran as high as 70%.¹² Patients and clinicians alike were crossing, through ordinary repeated contact, from tolerance into allergy, until latex stood among the leading causes of life-threatening allergic reactions in the operating room.
The response, when it finally came, didn’t cure anyone — it removed the exposure. Health authorities pushed hospitals toward powder-free and low-protein gloves, latex-safe operating rooms and supply chains, and synthetic substitutes; in 1997 the National Institute for Occupational Safety and Health issued a formal alert instructing employers how to protect workers,¹² and U.S. regulators began requiring every device containing natural rubber latex to carry a plain warning that it may cause allergic reactions.¹¹ It worked, and the proof is in what followed: where powder-free gloves became the rule, new sensitization among health workers fell toward zero, and the broad population rates that had reached several percent declined to a fraction of that.¹² The system was made to see the hazard, and once it could see it, it engineered it down.
Chlorhexidine fits that shape almost exactly — one stage earlier. It is ubiquitous, and its use is still expanding. The sensitivity to it is acquired through ordinary cumulative exposure. And it has already become a leading surgical allergen: in the United Kingdom’s national audit, chlorhexidine was behind about 9% of life-threatening perioperative anaphylaxis, while latex — the hazard that was engineered out — had all but vanished from the same tables.⁵ One material was made visible and brought to heel. The other is doing now what the first one did then, and is still, for the most part, unwatched.
The clearest measure of that is the labeling itself. Latex carries both a mandatory caution on medical devices¹¹ and a standardized hazard symbol that lets anyone identify it at a glance. Chlorhexidine has neither. In the U.K., safety leaders have had to petition international standards bodies to create a chlorhexidine symbol at all — pointing out, as grounds, that it is now a more common cause of anaphylaxis than latex ever was.⁹ Latex was made legible to the whole system. Chlorhexidine, by and large, still isn’t.
What to do while the system catches up
None of this resolves on the timescale of a single operation, and that is the hard part: the danger is here now, and the protection isn’t. We can’t hand you a system that watches for this. What we can hand you is the short list of things we wish someone had handed us — three widening circles, starting with the one that costs nothing and is for everyone.
For everyone, before any procedure: don’t shave or wax the area first. Freshly shaved or waxed skin is disrupted skin, and disrupted skin absorbs more of whatever is applied to it — including chlorhexidine, in the words of the case at the center of this piece.² We want to be honest about what that does and doesn’t buy you: it is not protection from a reaction. Chlorhexidine reaches the body through many routes, and skipping the razor closes only one of them. But it is one of the very few avenues you actually control, it costs nothing, and right now nothing in the system tells you about it. There isn’t even a rule. The closest thing — longstanding guidance that surgical sites not be shaved with a razor — is voluntary, unevenly followed, and written to prevent infection rather than to limit absorption; it says nothing about waxing at all.¹⁰ So treat it the way you already treat “nothing to eat after midnight before surgery”: a small, free habit everyone simply adopts, once someone finally says it out loud. And then say it out loud to the people you love. That part matters more than any single precaution — because the next person it protects may be someone who would otherwise never have heard it at all.
If you have ever reacted to it: if a surgical scrub, an antiseptic wipe, a chlorhexidine mouthwash, or a coated catheter ever left you with hives, a rash, or swelling, say so before your next procedure — and ask, plainly, whether a chlorhexidine-free preparation can be used. Alternatives exist, and they are routinely substituted when there’s a reason to.⁷ You don’t need a confirmed diagnosis to ask the question. The reaction worth preventing is the one that hasn’t happened yet.
And for the system that is supposed to be doing this work: the gaps are nameable, which is the same as saying they are fixable. Give chlorhexidine allergy a specific way to be recorded and counted, so confirmed cases stop dissolving into “anaphylaxis, cause unknown.” Make the allergy record stop the exposure — a hard interruption at the prep tray and the supply cabinet, not an alert that fires after the wipe is already open. Watch for it actively, the way a hazard of this size warrants. Label it, the way latex is labeled. Stock the alternatives and make them easy to reach. None of this is novel; it is, almost line for line, what was already done once — for latex.
We come back, at the end, to the morning this started. Katherine went in for a routine operation with no reason to think an antiseptic would be the thing that nearly killed her — because nothing in the system was built to tell her, or to catch it when it happened. She survived. Most of the people walking the same path don’t know they’re on it.
That’s the part we can’t stop thinking about. The danger here isn’t exotic. It’s ordinary — accumulating quietly in a population that meets chlorhexidine at a scale no one is counting, surfacing without warning, and recorded, when it’s recorded at all, as something else. The rarity was never real. It was the shape of a blind spot.
But blind spots can be closed; we’ve done it before. A generation ago we watched a ubiquitous material become a mass sensitivity crisis, and we made it visible — with labels, with defaults, with a hazard the whole system learned to see. Nothing chlorhexidine needs is beyond us. It’s the same work, on a hazard that has quietly grown larger, and the only thing missing is the decision to begin.
We’re not asking you to be afraid of your next surgery. We’re asking you to know what we didn’t: that the wipe, the rinse, the coated line are not nothing; that a reaction to an antiseptic is worth remembering and saying out loud; that you can skip the razor before a procedure and tell the people you love to do the same. Small things — but they’re the things the system hasn’t yet handed you.
We wrote this because the morning it happened to us, none of it was written down anywhere we could find. Now it is. If you’re reading because chlorhexidine has already hurt you or someone you love, you are not an anomaly in the data — you are the part of it that was never counted. And if you’re reading before anything has happened, you already know more than we did. That was the whole point.
REFERENCES
1. Dobson GP. Trauma of major surgery: A global problem that is not going away. International Journal of Surgery. 2020;81:47–54. doi.org/10.1016/j.ijsu.2020.07.017 Link: https://doi.org/10.1016/j.ijsu.2020.07.017
2. Husain MA, Pelz BJ. Perioperative chlorhexidine anaphylaxis [case poster]. Presented at the American College of Allergy, Asthma & Immunology (ACAAI) Annual Scientific Meeting, 2025; Medical College of Wisconsin. (Independent peer-presented case report. Venue and title line to be confirmed against the poster header before publication.)
(peer-presented case poster — no public link)
3. Marquart E, Kinaciyan T. Chlorhexidine: a hidden and often undeclared allergen. Allergo Journal International. 2025;34:271–275. doi.org/10.1007/s40629-025-00351-x Link: https://doi.org/10.1007/s40629-025-00351-x
4. Opstrup MS, Jemec GBE, Garvey LH. Chlorhexidine allergy: on the rise and often overlooked. Current Allergy and Asthma Reports. 2019;19:23. doi.org/10.1007/s11882-019-0858-2 Link: https://doi.org/10.1007/s11882-019-0858-2
5. Harper NJN, Cook TM, Garcez T, et al. Anaesthesia, surgery, and life-threatening allergic reactions: epidemiology and clinical features of perioperative anaphylaxis in the 6th National Audit Project (NAP6). British Journal of Anaesthesia. 2018;121(1):159–171. (See also NAP6 Report, Chapter 17: Chlorhexidine. Royal College of Anaesthetists, 2018, which records the 0.78-per-100,000 estimate and the ~one-quarter-suspected figure, and notes the rate is “likely an overestimate.”) bjanaesthesia.org Link: https://www.bjanaesthesia.org/article/S0007-0912(18)30318-0/fulltext
6. Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. Institute of Medicine. Washington, DC: National Academies Press; 2000. nap.nationalacademies.org Link: https://nap.nationalacademies.org/catalog/9728/to-err-is-human-building-a-safer-health-system
7. Attested clinical record — Asthma, Allergy & Clinical Immunology clinic, Children’s Wisconsin / Medical College of Wisconsin: clinic visit note (July 2, 2025) and physician letters (July 3, 2025; August 9, 2025). Documented medical record; not publicly linked.
(attested clinical record — not publicly linked)
8. U.S. Food and Drug Administration. Drug Safety Communication: FDA warns about rare but serious allergic reactions with the skin antiseptic chlorhexidine gluconate. February 2, 2017. (52 reports of anaphylaxis to topical chlorhexidine, 1969–2015; 43 drawn from FAERS; 2 fatal.) fda.gov Link: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-warns-about-rare-serious-allergic-reactions-skin-antiseptic
9. Safe Anaesthesia Liaison Group (SALG). Chlorhexidine allergy and devices. Patient Safety Update, January–June 2023. (UK proposal for a standardized chlorhexidine device-hazard symbol modeled on the latex symbol in ISO 15223-1; notes chlorhexidine is now a more common cause of anaphylaxis than latex.) salg.ac.uk Link: https://www.salg.ac.uk/salg-publications/patient-safety-update/patient-safety-update-january-june-2023/chlorhexidine-allergy-and-devices/
10. Centers for Disease Control and Prevention. Guideline for Prevention of Surgical Site Infection, 1999. Infection Control & Hospital Epidemiology. 1999;20(4):247–278. World Health Organization. Global Guidelines for the Prevention of Surgical Site Infection. 2016. (Both discourage preoperative razor shaving — advising clippers or no hair removal — for infection-control reasons.)
(CDC 1999 SSI guideline + WHO 2016 SSI guideline — no single link)
11. U.S. Food and Drug Administration. User labeling for devices that contain natural rubber. 21 CFR §801.437 (final rule 1997; effective 1998). (Mandatory bold allergy caution on devices containing natural rubber latex; no analogous chlorhexidine requirement exists.) ecfr.gov Link: https://www.ecfr.gov/current/title-21/chapter-I/subchapter-H/part-801/subpart-H/section-801.437
12. National Institute for Occupational Safety and Health (NIOSH). Preventing Allergic Reactions to Natural Rubber Latex in the Workplace. NIOSH Alert, Publication No. 97-135. Cincinnati, OH: U.S. Department of Health and Human Services; June 1997. (Documents the latex-allergy epidemic following the adoption of universal precautions, the role of cornstarch glove powder in aerosolizing latex protein, and the powder-free/low-protein interventions that reduced sensitization. Peak prevalence figures — up to ~17% of health care workers and ~70% of patients with spina bifida, with declines following powder-free and latex-safe measures — drawn from Katelaris CH, “Latex Allergy: Diagnosis and Management,” World Allergy Organization, updated 2022.) cdc.gov/niosh
Link: https://www.cdc.gov/niosh/docs/97-135/
By Kenneth Hoffmann and Katherine Hoffmann Goldsword, Founders · Hoffmann Goldsword Foundation.
© 2025–2026 Hoffmann Goldsword LLC · Licensed to the Hoffmann Goldsword Foundation · Published under CC BY-NC-SA 4.0 — https://creativecommons.org/licenses/by-nc-sa/4.0/ · HoffmannGoldsword.org
Commercial use or syndication requires a separate license from Hoffmann Goldsword LLC — MediaGroup@HoffmannGoldsword.com